The natural history of recovery from psychological trauma:
a therapeutic model.
Philip V. Dutton
Retired Consultant Clinical Psychologist,
Consultant Neurosomatic Psychotherapist, Edinburgh, Scotland UK
Andrew J. Ashworth
General Medical Practitioner, Bonhard House, Bonhard Medical Limited,
Bo’ness, Scotland UK
Abstract
A modified Psychological Trauma Recovery Model is described.
It includes four dynamic levels to identify intervention opportunities and relapse risks for improved shaping of therapy.
Introduction
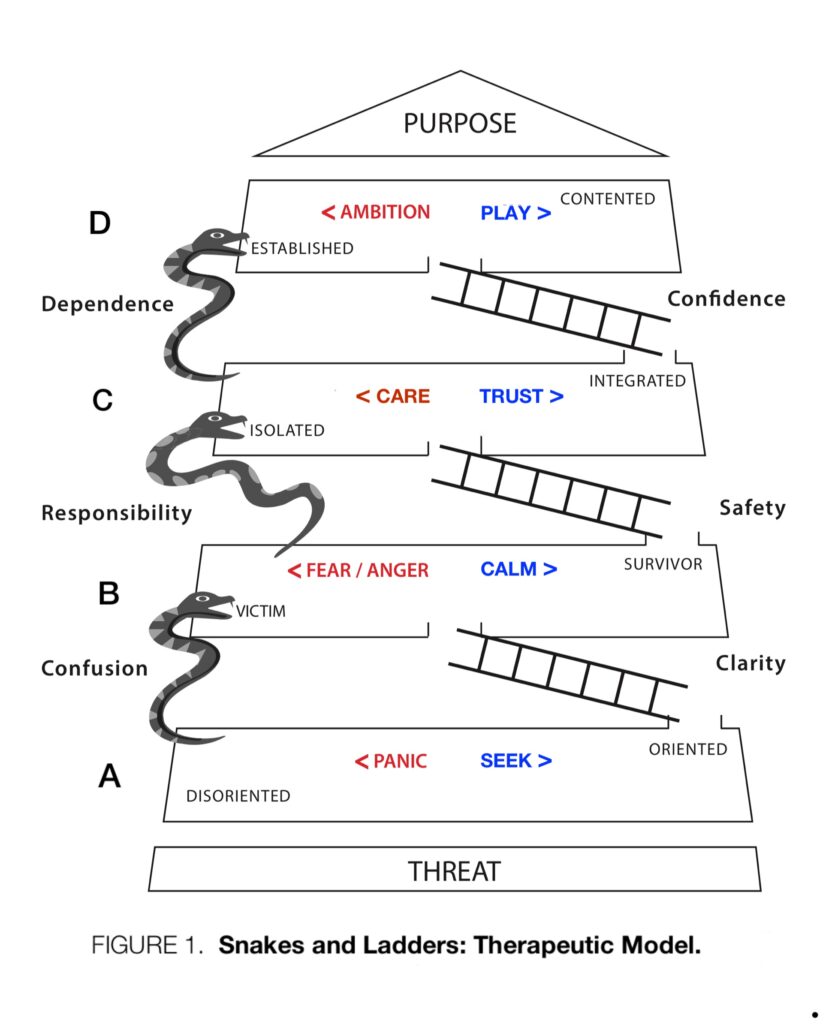
Dutton & Ashworth [1] presented a theoretical paradigm on the natural recovery history from psychological trauma involving subjects’ feelings, emotions, and drives. Using this descriptive model in clinical practice has helped to identify therapeutic objectives and relapse risks at various levels (A B C D Figure 1). Patient feedback has facilitated modifications and refinement of the model to share with patients, guide therapy and monitor progress.
Hypothesis
Therapeutic interventions following trauma can be readily and quickly chosen and reviewed with informed patient input using a visual aid for practical assessment and communication.
Extended Paradigm
The original Dutton Ashworth [1] model was based on Panksepp’s seven basic affective systems [2]. Panksepp’s terminology was modified: ‘Rage’ was relabelled as ANGER and ‘Lust’ as AMBITION.
Clinical experience using this SnakesandLadders model led to the pairing of FEAR and ANGER affective drives because they were responsive to the same treatments and had similar neurobiological foundations [3].
CALM drives attenuate FEAR and ANGER, permitting a feeling of safety. In practice, accepting Responsibility for the CARE of others led to an ISOLATEDemotional state. TRUST (accepting CARE from others and the self) encouraged an INTEGRATED emotional state [4].
The therapeutic objectives (ladders) of Clarity, Safety and Confidence are defined. The relapse risks (Snakes) of Dependence, Responsibility and Confusion are identified. PURPOSE replaces Hope as an appropriate representation of self-actualisation.
Discussion:
Using the original model [1] with patients/clients allowed adjustment and extension of the therapeutic approach from their feedback—[Figure 1].
Using this new model, patients described which of three cycles of recovery and relapse they found themselves in. The cycles corresponded with the stages of The Transtheoretical Model of Change [5]. In the Snakes and Ladders model, the cycles have been labelled according to the therapeutic objectives (Ladders) of Clarity, Safety and Confidence and associated relapse risks: (Snakes) of Confusion, Responsibility and Dependence.
This hierarchical description has aided patient orientation in recovery and relapse and enabled targeted therapeutic intervention.
Patient Journey – (relating to Figure 1)
Horizontal moves. Patients present on the regressive (left) side of the model (in levels A-D), driven by PANIC, FEAR/ANGER, or CARE and then, either naturally or encouraged by therapy, progress via drives of SEEK, CALM or TRUST. The fourth drive, PLAY, reflects relapse prevention.
Vertical moves. Upward transitions between levels are represented by the Ladders and are automatic and rapid (as in the board game). Thus an ORIENTED person achieves Clarity (about the threat) and progresses to VICTIM status. Similarly, a SURVIVOR recognises Safety from the Threat and becomes ISOLATED, whilst an INTEGRATED person develops Confidence to become ESTABLISHED and eventually CONTENTED, achieving Purpose.
Downward transitions represented by Snakes are similarly rapid. They are perceived as attractive compared to the uncertainty and difficulty of progress. Thus Confusion appeals to a VICTIM by giving respite to FEAR/ANGER. Feeling Responsibility (e.g. guilt) becomes attractive when ISOLATED by declining CARE. Dependence becomes attractive when ESTABLISHED, avoiding the responsibility of AMBITION.
Therapeutic interventions
Therapeutic objectives in this model are based on encouraging horizontal progress from left to right, with vertical changes following automatically (up a ladder).
Relapse (sliding down a Snake) is perceived as attractive. Therefore, understanding the nature of relapse, its precursors and consequences helps focus on appropriate positive drives, necessary for progress.
Conclusion
This model permits patients and therapists to understand and identify the most appropriate interventions at each stage of their therapeutic journey.
References
[1] Dutton P. V. & Ashworth A. J.
The natural history of recovery from psychological trauma: An observational model.
Medical Hypotheses 85 (2015) 588–590; 2015.
[2] Panksepp J, & Biven L. The archaeology of mind: neuroevolutionary origins of human emotions. Norton Series on Interpersonal Neurobiology; 2012.
[3] Ashworth A. J. & Dutton P. V.
BabyGaze: A Rapid Neurobiological Intervention for Anxiety, Panic and Anger
Int J Psychiatry, 2017 ISSN: 2475-5435; 2017.
(http://www.opastonline.com/wp-content/uploads/2017/08/babygaze-a-rapid- neurobiological-intervention-for-anxiety-panic-and-anger-IJP-17-026.pdf)
[4] Bowlby, John. Attachment and Loss Volume I Attachment (Second Edition)
Basic Books (Tavistock Institute of Human Relations) 1969, 1982
[5] Prochaska J O and DiClemente, C C
Stages and Processes of Self-Change of Smoking: Toward An Integrative Model of Change
Journal of Consulting and Clinical Psychology, Vol. 51, No. 3, 390-395; 1983.
Acknowledgements
We thank our Patients for their assistance in the development of this model.
Gareth Villis of Zen Visual for the ‘Snakes and Ladders’ illustration (Figure 1).
First written in 2017 – no known conflicts of interest.
First published independently by P V Dutton and A. J Ashworth 2022.